A synthetic tricyclic derivative of carboxamide with antineoplastic activity.
MECHANISM OF ACTION:
Lonafarnib is a non-peptidomimetic inhibitor of farnesyl transferase, an enzyme responsible for
the post-translational lipid modification of a wide variety of cellular proteins that are involved in
the pathogenic pathways of various diseases including cancer and progeria.
Lonarfanib binds to and inhibits farnesyl transferase, an enzyme involved in the post-translational modification and activation of Ras proteins. Ras proteins participate in numerous signalling pathways (proliferation, cytoskeletal organization), and play an important role in oncogenesis. Mutated ras proteins have been found in a wide range of human cancers and progeria. Isoprenylation involves the enzyme farnesyltransferase (FTase) transferring a farnesyl group from farnesyl pyrophosphate (FPP) to the pre-Ras protein.(The membrane targeting COOH-terminal CAAX box (C = cysteine, A = aliphatic, X = any amino acid) is first prenylated followed by AAX proteolysis, carboxymethylation, and palmytoylation. These steps of posttranslational modification are of importance for the membrane tethering of Ras proteins. Icmt,isoprenylcysteine carboxyl methyltransferase; lys, lysine; P-P, PPI; PTI, prenyl transferase inhibitor; Rce1,Ras-converting enzyme 1.)
PHARMAKOKINETICS OF LONAFARNIB:
Nineteen patients had samples collected for pharmacokinetic evaluations. Lonafarnib was slowly absorbed after oral administration with food. Median Tmax ranged from 3 to 8 h. oral administration of lonafarnib with food. Mean plasma lonafarnib concentrations at 12 h after the dose were ∼34–99% of the corresponding mean Cmax values. The mean total body clearance ranged from 165 to 364 ml/min. No effect of food on pnarmacokinetics.
SIDE EFFECTS:
Mild diarrhea, fatigue, nausea, vomiting, anorexia,depressed serum hemoglobin,fever,Dehydration, Constipation, Hypokalemia
Lonafarnib side effect was reported by a Health Professional from UNITED STATES on June
28, 2006. Male patient, 50 years of age, weighting 136.0 lb, was diagnosed with adenocarcinoma and was treated with Lonafarnib. After drug was administered, patient experienced the following side effects: cardiac arrest , diarrhoea,hypotension,hypovolaemia, nausea , pancytopenia,sepsis.
Lonafarnib dosage: 150 MG PO BID. During the same period patient was treated with
DOCETAXEL, DURAGESIC, DECADRON, SYNTHROID, ZOFRAN.
CANCER:
Although extensive clinical research indicates limited activity of lonafarnib in solid tumors, there
is recent interest in combinations of farnesyl transferase inhibitors with imatinib or bortezomib in hematological malignancies.The initial expectations of specificity of FTIs for cells with ras mutations matched the original in vitro observations. However, subsequent in vitro and in vivo studies demonstrated that FTI-mediated inhibition of tumor growth was not tightly linked to rasmutation status. It is now clear that ras mutation is not a requirement for FTI effects on tumor cells. It has not, however, been shown that Ras signaling inhibition does not play a role in these effects.FTIs showed significant promise in preclinical studies. On the other hand, these studies also showed that there was tumor regrowth after treatment cessation in mice and that FTIs alone were not curative. The relatively poor response rates reported in clinical trials with FTIs alone might be explained by these preclinical results. However, combination of FTIs with other
therapies may have a good potential, if these are applied according to biological principals of
activity.
In using FTIs in combined modality treatment, the timing of FTI administration relative to chemo-
or radiotherapy may be critical. As discussed above, not every chemotherapeutic drug will be
suitable for combination with FTIs. The combination of FTIs with radiation is, in our experience,
well tolerated and engenders no additional radiation toxicity to normal tissues. The Phase I trial
of L-778,123 with radiation yielded encouraging results for this combination, consistent with our
preclinical findings. This may result from a combination of FTI effects on tumor cell radiosensitivity, perhaps via inhibition of PI3K activation, and effects on the tumor microenvironment as well as the antiproliferative effects of FTIs.
Phase I and II clinical trials confirmed relevant antitumour activity and low toxicity; however, no
improvement in overall survival has been reported in Phase III trials.
PROGERIA:
Progeria, also known as Hutchinson-Gilford Progeria Syndrome (HGPS), is a rare, fatal genetic disease characterized by an appearance of accelerated aging in children.Twenty-eight children from sixteen countries participated in the two-and-a-half year drug trial,representing 75 percent of known Progeria cases worldwide at the time the trial began. Of those, 26 are children with the classic form of Progeria.Researchers also examined arterial stiffness (a predictor of heart attack and stroke in the general population), bone density and rigidity (indicators of osteoporosis). Every child completing the study showed improvement in an ability to gain additional weight, increased flexibility of blood vessels or improved bone structure.
Results included improvement in one or more of the following areas:
Weight: One in three children demonstrated a greater than 50 percent increase in annual rate of weight gain or switched from weight loss to weight gain, due to increased muscle and bone mass.
Bone Structure: On average, skeletal rigidity (which was highly abnormal at trial initiation) improved to normal levels after FTI treatment.
Cardiovascular: Arterial stiffness, strongly associated with atherosclerosis in the general aging population, decreased by 35 percent. Vessel wall density also improved with treatment.
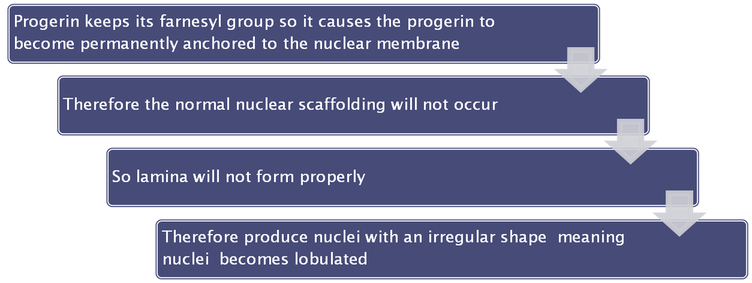
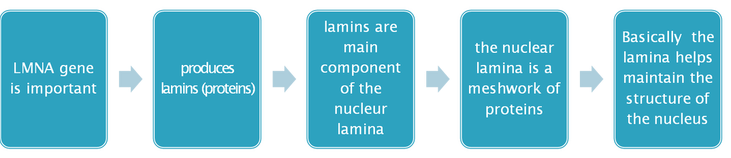
Following the 2003 discovery of the gene that causes Progeria, researchers identified FTIs as a potential drug treatment for Progeria. Children with Progeria have a genetic mutation that leads to the production of the protein progerin, which is responsible for Progeria. Progerin blocks normal cell function and part of its toxic effect on the body is caused by a molecule called a "farnesyl group," which attaches to the progerin protein. FTIs act by blocking the attachment of the farnesyl group onto progerin.
REFERENCES:
1.Thomas B. Brunner, Stephen M. Hahn, Anjali K. Gupta, Ruth J. Muschel,W. Gillies McKenna,
and Eric J. Bernhard;Farnesyltransferase InhibitorsAn Overview of the Results of Preclinical and Clinical Investigations; Cancer Res September 15,2003 63; 5656
2. Fadlo R. Khuri 1 , Bonnie S. Glisson 2 , Edward S. Kim 2 , Paul Statkevich 3 ,Peter F.
Thall 2 , Michael L. Meyers 3 , Roy S. Herbst 2 , Reginald F. Munden 2 ,Craig Tendler 3 , Yali
Zhu 3 , Sandra Bangert 2 , Elizabeth Thompson 2 ,Charles Lu 2 , Xue-Mei Wang 2 , Dong M.
Shin 2 , Merrill S. Kies 2 ,Vali Papadimitrakopoulou 2 , Frank V. Fossella 2 , Paul Kirschmeier 3 ,W.Robert Bishop 3 , and Waun Ki Hong ;Phase I Study of the Farnesyltransferase Inhibitor
Lonafarnib with Paclitaxel in Solid Tumors; Cancer Res May 1, 2004 10;2968
3. Lonafarnib for cancer and progeria, Wong NS,Morse MA, 2012 Jul;21(7):1043-55. doi:10.1517/13543784.2012.688950.Epub 2012 May 24.Morse MA.
4.http://cancerres.aacrjournals.org
5.http://www.pnas.org/content/suppl/2012/09/18/1202529109.DCSupplemental/pnas.2012022
9SI.pdf#nameddest=ST1
6.http://www.news-medical.net
7.www.progeriaresearch.org
8.www.ncbi.nlm.nih.gov/pubmed/22620979
9.clinicaltrials.gov/ct2/show/NCT00425607
MECHANISM OF ACTION:
Lonafarnib is a non-peptidomimetic inhibitor of farnesyl transferase, an enzyme responsible for
the post-translational lipid modification of a wide variety of cellular proteins that are involved in
the pathogenic pathways of various diseases including cancer and progeria.
Lonarfanib binds to and inhibits farnesyl transferase, an enzyme involved in the post-translational modification and activation of Ras proteins. Ras proteins participate in numerous signalling pathways (proliferation, cytoskeletal organization), and play an important role in oncogenesis. Mutated ras proteins have been found in a wide range of human cancers and progeria. Isoprenylation involves the enzyme farnesyltransferase (FTase) transferring a farnesyl group from farnesyl pyrophosphate (FPP) to the pre-Ras protein.(The membrane targeting COOH-terminal CAAX box (C = cysteine, A = aliphatic, X = any amino acid) is first prenylated followed by AAX proteolysis, carboxymethylation, and palmytoylation. These steps of posttranslational modification are of importance for the membrane tethering of Ras proteins. Icmt,isoprenylcysteine carboxyl methyltransferase; lys, lysine; P-P, PPI; PTI, prenyl transferase inhibitor; Rce1,Ras-converting enzyme 1.)
PHARMAKOKINETICS OF LONAFARNIB:
Nineteen patients had samples collected for pharmacokinetic evaluations. Lonafarnib was slowly absorbed after oral administration with food. Median Tmax ranged from 3 to 8 h. oral administration of lonafarnib with food. Mean plasma lonafarnib concentrations at 12 h after the dose were ∼34–99% of the corresponding mean Cmax values. The mean total body clearance ranged from 165 to 364 ml/min. No effect of food on pnarmacokinetics.
SIDE EFFECTS:
Mild diarrhea, fatigue, nausea, vomiting, anorexia,depressed serum hemoglobin,fever,Dehydration, Constipation, Hypokalemia
Lonafarnib side effect was reported by a Health Professional from UNITED STATES on June
28, 2006. Male patient, 50 years of age, weighting 136.0 lb, was diagnosed with adenocarcinoma and was treated with Lonafarnib. After drug was administered, patient experienced the following side effects: cardiac arrest , diarrhoea,hypotension,hypovolaemia, nausea , pancytopenia,sepsis.
Lonafarnib dosage: 150 MG PO BID. During the same period patient was treated with
DOCETAXEL, DURAGESIC, DECADRON, SYNTHROID, ZOFRAN.
CANCER:
Although extensive clinical research indicates limited activity of lonafarnib in solid tumors, there
is recent interest in combinations of farnesyl transferase inhibitors with imatinib or bortezomib in hematological malignancies.The initial expectations of specificity of FTIs for cells with ras mutations matched the original in vitro observations. However, subsequent in vitro and in vivo studies demonstrated that FTI-mediated inhibition of tumor growth was not tightly linked to rasmutation status. It is now clear that ras mutation is not a requirement for FTI effects on tumor cells. It has not, however, been shown that Ras signaling inhibition does not play a role in these effects.FTIs showed significant promise in preclinical studies. On the other hand, these studies also showed that there was tumor regrowth after treatment cessation in mice and that FTIs alone were not curative. The relatively poor response rates reported in clinical trials with FTIs alone might be explained by these preclinical results. However, combination of FTIs with other
therapies may have a good potential, if these are applied according to biological principals of
activity.
In using FTIs in combined modality treatment, the timing of FTI administration relative to chemo-
or radiotherapy may be critical. As discussed above, not every chemotherapeutic drug will be
suitable for combination with FTIs. The combination of FTIs with radiation is, in our experience,
well tolerated and engenders no additional radiation toxicity to normal tissues. The Phase I trial
of L-778,123 with radiation yielded encouraging results for this combination, consistent with our
preclinical findings. This may result from a combination of FTI effects on tumor cell radiosensitivity, perhaps via inhibition of PI3K activation, and effects on the tumor microenvironment as well as the antiproliferative effects of FTIs.
Phase I and II clinical trials confirmed relevant antitumour activity and low toxicity; however, no
improvement in overall survival has been reported in Phase III trials.
PROGERIA:
Progeria, also known as Hutchinson-Gilford Progeria Syndrome (HGPS), is a rare, fatal genetic disease characterized by an appearance of accelerated aging in children.Twenty-eight children from sixteen countries participated in the two-and-a-half year drug trial,representing 75 percent of known Progeria cases worldwide at the time the trial began. Of those, 26 are children with the classic form of Progeria.Researchers also examined arterial stiffness (a predictor of heart attack and stroke in the general population), bone density and rigidity (indicators of osteoporosis). Every child completing the study showed improvement in an ability to gain additional weight, increased flexibility of blood vessels or improved bone structure.
Results included improvement in one or more of the following areas:
Weight: One in three children demonstrated a greater than 50 percent increase in annual rate of weight gain or switched from weight loss to weight gain, due to increased muscle and bone mass.
Bone Structure: On average, skeletal rigidity (which was highly abnormal at trial initiation) improved to normal levels after FTI treatment.
Cardiovascular: Arterial stiffness, strongly associated with atherosclerosis in the general aging population, decreased by 35 percent. Vessel wall density also improved with treatment.
Following the 2003 discovery of the gene that causes Progeria, researchers identified FTIs as a potential drug treatment for Progeria. Children with Progeria have a genetic mutation that leads to the production of the protein progerin, which is responsible for Progeria. Progerin blocks normal cell function and part of its toxic effect on the body is caused by a molecule called a "farnesyl group," which attaches to the progerin protein. FTIs act by blocking the attachment of the farnesyl group onto progerin.
REFERENCES:
1.Thomas B. Brunner, Stephen M. Hahn, Anjali K. Gupta, Ruth J. Muschel,W. Gillies McKenna,
and Eric J. Bernhard;Farnesyltransferase InhibitorsAn Overview of the Results of Preclinical and Clinical Investigations; Cancer Res September 15,2003 63; 5656
2. Fadlo R. Khuri 1 , Bonnie S. Glisson 2 , Edward S. Kim 2 , Paul Statkevich 3 ,Peter F.
Thall 2 , Michael L. Meyers 3 , Roy S. Herbst 2 , Reginald F. Munden 2 ,Craig Tendler 3 , Yali
Zhu 3 , Sandra Bangert 2 , Elizabeth Thompson 2 ,Charles Lu 2 , Xue-Mei Wang 2 , Dong M.
Shin 2 , Merrill S. Kies 2 ,Vali Papadimitrakopoulou 2 , Frank V. Fossella 2 , Paul Kirschmeier 3 ,W.Robert Bishop 3 , and Waun Ki Hong ;Phase I Study of the Farnesyltransferase Inhibitor
Lonafarnib with Paclitaxel in Solid Tumors; Cancer Res May 1, 2004 10;2968
3. Lonafarnib for cancer and progeria, Wong NS,Morse MA, 2012 Jul;21(7):1043-55. doi:10.1517/13543784.2012.688950.Epub 2012 May 24.Morse MA.
4.http://cancerres.aacrjournals.org
5.http://www.pnas.org/content/suppl/2012/09/18/1202529109.DCSupplemental/pnas.2012022
9SI.pdf#nameddest=ST1
6.http://www.news-medical.net
7.www.progeriaresearch.org
8.www.ncbi.nlm.nih.gov/pubmed/22620979
9.clinicaltrials.gov/ct2/show/NCT00425607



{kind=link}